
Most readers who come across this text have one question in mind: is what just happened dangerous and do I need to go to the hospital. The short answer is: a marten bite is usually not a drama, but it is also never just a simple scratch — a bite wound from a wild predator behaves differently than a scraped knee, and the medical procedure is clear and simple.
This guide assumes the incident has already occurred. It shows what to do in the following minutes and hours, what biological risks are actually at play, when to head to the ER without discussion, and how to proceed if the victim is a dog or cat. If you previously only suspected that a marten was hanging around the property, this text is an emergency point, not a prevention guide.
§ 01Will a marten even bite a human?
Let's start with the most important part: the stone marten (Martes foina) does not attack humans. It is shy, territorial, and almost always chooses flight over confrontation. Statistics from rehabilitation centers and regional veterinary inspectorates are clear: in Poland, only a few to a few dozen marten bites are reported annually — most during attempts to catch it, remove it from an attic, or release it from a trap.
Situations in which a bite actually occurs fall into several scenarios:
- Catching the animal with bare hands — the most common reason. A panicked marten defends itself immediately, and its teeth can pierce standard gardening gloves.
- Defending the litter — between April and July, a female can attack unexpectedly if you get too close to a nest in an attic or woodpile.
- Sick or injured animal — an individual with an injury, in shock, or with neurological symptoms (potentially rabies, though rare) loses its normal flight distance.
- Conflict with a dog or cat — a person trying to separate fighting animals gets bitten accidentally, often on the hand or forearm.
- Inexperienced young — in early summer, young martens can be surprisingly incautious and may bite out of pure curiosity if you try to touch them.
The practical conclusion is that the risk of a bite increases in direct proportion to how close you get. Observing a marten from a distance is safe. Attempts at contact are not. We write more about its habits in the text Habits of the stone marten.
§ 02First aid — step by step
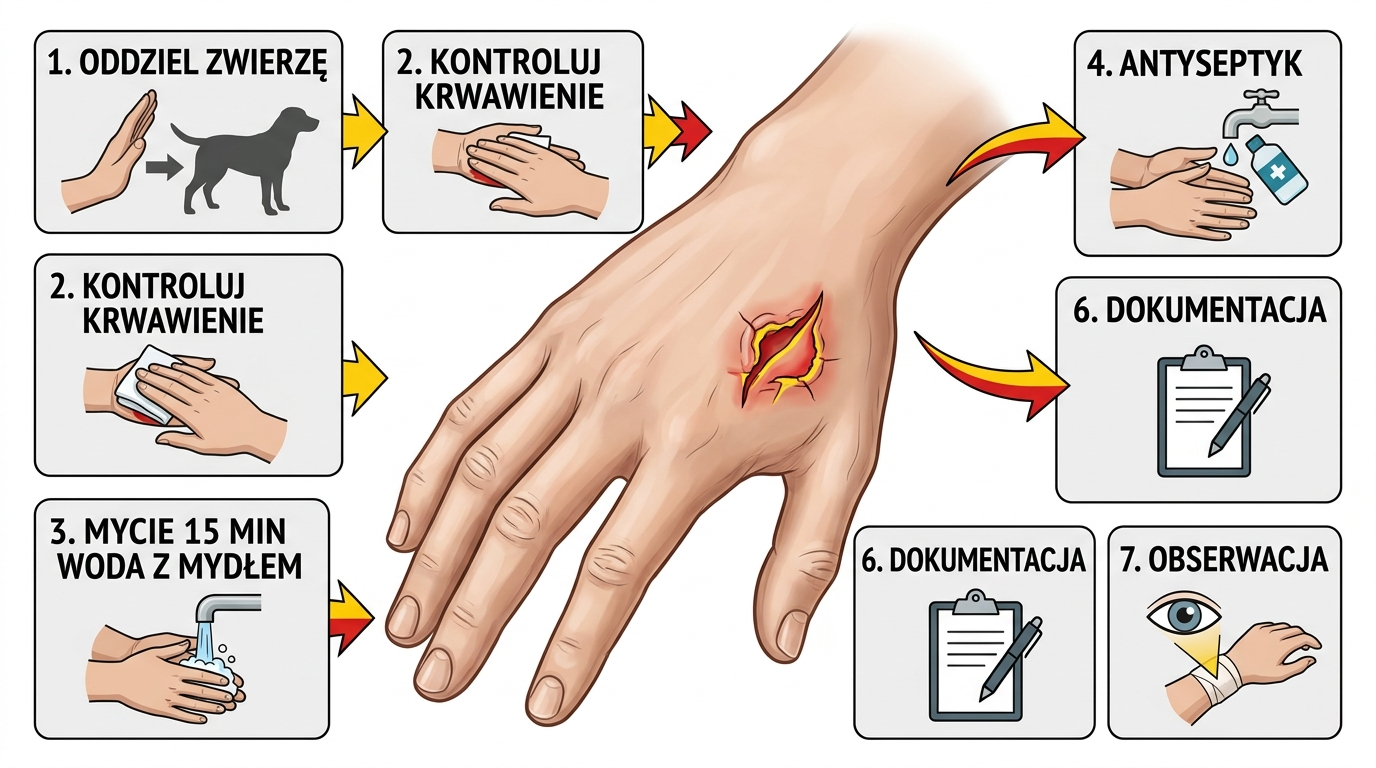
The procedure is the same for any bite from a wild mammal: bleeding control, thorough washing, antiseptic, dressing, documentation. The order and timing are important — the first 15 minutes are the best time to reduce the risk of infection by an order of magnitude. The later you wash the wound, the less effective all subsequent steps will be.
- Step 1 — calm the situation, separate the animal. Before doing anything to the wound, make sure the marten cannot bite again. Close it in a room or step back to a safe distance. A second bite while treating the first is not uncommon.
- Step 2 — bleeding control. Light to moderate bleeding from a bite wound is desirable — it flushes pathogens out of the bite canal. Do not stop it immediately with pressure. Only with heavy, pulsating bleeding (rare with martens because the teeth are small) apply pressure with clean gauze and elevate the limb.
- Step 3 — wash with soap and water for 10–15 minutes. This is the most important part of the entire procedure. Lukewarm, running water with soap (regular, kitchen, or gray soap), stream directed straight into the wound, massage the area. Do not cut it short — 15 minutes, measured by the clock. Soap breaks down bacterial envelopes and significantly reduces the risk of infection.
- Step 4 — antiseptic. After washing and drying with a clean towel, apply an antiseptic preparation: octenidine with phenoxyethanol (Octenisept, Octenilin) or povidone-iodine (Betadine). Alcohol and hydrogen peroxide are less recommended — they irritate tissues and delay healing. Leave to dry.
- Step 5 — loose, non-occlusive dressing. Sterile gauze, a plaster with a pad, a light bandage. Do not seal the wound tightly and do not use hydrocolloid plasters — bite wounds need air access, and occlusion promotes the multiplication of anaerobes (e.g., Clostridium tetani).
- Step 6 — documentation. Take a photo of the wound immediately and repeat after 12 and 24 hours. Note the date, time of the event, and circumstances (whether the animal was aggressive without reason, looked sick, or escaped). This is information the doctor will ask for.
- Step 7 — observation in the first 24 hours. Check the wound every few hours. Increasing swelling, redness extending beyond the wound edge, pus, warmth, pulsating pain, fever, red streaks running toward the heart — any of these symptoms mean go to the doctor now.
This guide does not replace medical consultation. In case of any doubts — wound depth, location on the face or hand, rapidly increasing swelling, unclear vaccination status, the victim is a child — immediately contact a GP, out-of-hours clinic, or the Emergency Room (ER). Indications for PEP (rabies post-exposure prophylaxis) are determined exclusively by a doctor after evaluating the exposure.
§ 03Biological risks — what we are actually afraid of
A bite wound from a wild predator differs from a knife cut in three ways: it is deep and narrow (teeth sink in like needles, creating a deep canal difficult to flush), it is contaminated with the animal's oral flora (rich and aggressive), and it is often accompanied by tissue crushing (locally weakened immune system in the wound area). These three factors together explain why bites become infected much more often than standard wounds.
Three risks that are always considered:
- Pasteurella multocida — a Gram-negative rod present in the oral cavity of practically all predatory mammals. It causes rapidly increasing local infection (redness, swelling, pain, pus) within 6–24 hours of the bite. In more severe cases, it leads to phlegmon, tendonitis, osteomyelitis, and exceptionally to sepsis. The standard first-line antibiotic is amoxicillin with clavulanic acid.
- Tetanus (Clostridium tetani) — bacterial spores common in soil, dust, and on animal teeth. Any deep, dirty wound with possible contamination is a potential entry point for infection. The disease (up to 3 weeks after the bite) is dangerous and costly to treat. Prevention through vaccination is incredibly simple — but only if you remember it.
- Rabies (rabies) — a virus transmitted by saliva through a bite or contact with a mucous membrane. In Poland, it is rare, but real. Poland is not officially a country free of wild animal rabies; in some provinces (mostly eastern), cases are recorded every few years in foxes, deer, and bats. Mustelids (marten, weasel, polecat) have been described as secondary carriers. Once symptoms appear in humans, the disease is 100% fatal, but post-exposure prophylaxis (PEP) given in the appropriate time window provides 100% protection.
For context: bacterial wound infections after a marten bite are a real scenario in fifteen to twenty percent of cases without proper first aid. Tetanus — with an up-to-date vaccination, practically zero risk. Rabies — in Polish reality, only a few exposure cases per year, but the consequences of oversight are serious enough that every bite by a wild animal is treated as a suspicious exposure by default until a doctor decides otherwise.
§ 04When to absolutely see a doctor or go to the ER
For some readers, the news will be inconvenient, but it is unambiguous: after a bite by a wild animal, contacting a doctor is standard, not over-caution. In mild cases, this can be a visit to a GP within 24 hours. In more serious cases — the ER on the same day, preferably within 6 hours.
| Situation / symptom | Reaction |
|---|---|
| Small superficial bite, adult, vaccinations up to date | GP within 24 h, wound check |
| Deep bite wound, bleeding difficult to stop | ER immediately |
| Location: face, neck, hand, joint | ER immediately (functional and aesthetic risk) |
| Victim: child under 12 or elderly person | ER immediately |
| Victim: pregnant woman, immunocompromised person | ER immediately |
| Animal escaped or looked sick (drooling, disorientation) | ER — rabies PEP assessment |
| No tetanus vaccination within the last 5+ years | ER or clinic within 24 h — booster |
| Wound after 12–24 h: swelling, redness, pus, fever | ER / out-of-hours, antibiotic therapy |
| Red streaks from wound toward heart, fever, chills | ER immediately — suspected sepsis |
Location matters more than it seems at first glance. The hand is a dense network of tendons, sheaths, and small joints — infection spreads through them rapidly and can lead to permanent limitation of finger mobility within 48 hours. The face — proximity to airways, eyes, and vessels. Joints — the risk of septic arthritis requires rapid surgical evaluation. These three areas are treated with a separate standard.
Go to the ER without discussion if: the wound is on the face, hand, or joint; the victim is a child, pregnant woman, or immunocompromised; bleeding is hard to stop; the animal disappeared or looked sick (PEP risk); symptoms of systemic infection appear — fever, chills, increasing swelling, red streaks. It's not worth waiting until morning — antibiotic therapy started after 24 hours is twice as less effective as that started after 6.
§ 05Vaccines — tetanus and rabies prophylaxis (PEP)
Two vaccines that will be discussed in the doctor's office after a marten bite: anti-tetanus (routinely, for every bite wound) and anti-rabies in the post-exposure schedule (PEP) (conditionally, after risk assessment).
The tetanus vaccine is not a reaction to an incident — it is the background that you either have or you don't. Remember it before, not just after.
Tetanus. The Polish vaccination schedule includes full tetanus vaccination in childhood, with booster doses at ages 6, 14, and 19. In adults, a booster dose every 10 years is recommended. After a bite, the doctor asks for the date of the last vaccination. The shortened scheme is:
- Vaccination up to date (last dose < 5 years ago) — usually no additional dose is given if the wound is clean and superficial.
- Vaccination 5–10 years ago — booster dose (Td or Tdap), 1 injection.
- Vaccination over 10 years ago or not remembered — booster dose + possibly tetanus immunoglobulin (for deep, dirty, bite wounds).
- No documented vaccination in the past — full primary vaccination schedule (3 doses) plus immunoglobulin.
Rabies — PEP (Post-Exposure Prophylaxis). The rule is simple: if the animal cannot be observed (it escaped, was killed, was wild), the exposure is treated as suspicious and prophylaxis is implemented. PEP in the Essen schedule includes five doses of the vaccine (days 0, 3, 7, 14, 28). For deep wounds, facial wounds, or for previously unvaccinated victims — specific immunoglobulin is additionally administered around the wound on day zero.
Practically speaking: PEP is effective if implemented before symptoms appear. The earlier, the better — the standard is to start within 24–48 hours of exposure. After rabies symptoms appear in humans, treatment is practically ineffective. The decision regarding PEP is always made by a doctor based on exposure assessment and the epidemiological situation in the specific district.
Take to the ER (or the doctor's office): vaccination card or medical records with the date of the last tetanus vaccination, photos of the wound from the moment of the incident, and a brief description of the circumstances (what you were doing, if the animal was aggressive without reason, if it escaped, if anyone saw it). These three pieces of information cut the assessment time in half.
§ 06Dog or cat bitten by a marten
Another common scenario: a marten bit your dog or cat. Most often this happens at night in the garden when a dog tries to catch a marten by the composter or a cat gets into a fight near the chicken coop. From a veterinary point of view, the rule is simple: veterinarian on the same day, regardless of how the wound looks. There are two reasons: bacterial risk and rabies risk.
What to do before you reach the clinic:
- Safely separate the animals — a dog stimulated by a fight can still be dangerous to humans. Wear thick gloves when approaching the wound.
- Check general condition — is the animal walking normally, does it have shortness of breath, is it limping? Bleeding from a wound in the neck, chest, or abdomen area — particular urgency.
- Moderate bleeding — rinse with sterile saline (buy at a pharmacy, small bottle) or boiled water; do not use human antiseptics, some (e.g., alcohol) irritate the mucous membranes and subcutaneous tissue of animals.
- Light protective dressing — gauze and bandage, if the animal allows. Do not tie the limb or neck tightly.
- Transport in a carrier or on a leash — directly to the nearest on-duty veterinarian. In apps like Petsy, Vetsi, or searching '24h veterinary clinic', you will find the nearest address.
At the clinic, the doctor will assess the depth of the wound, decide on sedation and surgical debridement (bite wounds usually require cleaning, sometimes drainage, rarely primary suturing — anaerobes!), implement antibiotic therapy, and decide on a rabies booster vaccination.
If your dog or cat does not have an up-to-date rabies vaccination and was bitten by a wild animal, the situation becomes a formal epidemiological problem. The animal should be revaccinated immediately, and the regional veterinarian usually imposes mandatory observation lasting up to 6 months (in extreme cases, euthanasia). An up-to-date rabies vaccine for a dog is a legal requirement in Poland — and one of the best 50 PLN investments you can make.
§ 07Prevention — how not to get bitten
The best dressing is the one that doesn't need to be applied. In practice, 80% of marten bites that end up in statistics are completely avoidable incidents — a moment of thought and a few simple rules would suffice.
- Do not catch a marten with bare hands. Not with bare hands, and not with thin gardening gloves. Marten teeth pierce regular leather with zero resistance. If you must move the animal — use a transport crate, a long pole, and thick two-layer protective gloves (leather plus fabric).
- Do not put your hands into woodpiles, between joists, or into roof gaps if you know a marten is present on the property. Especially in spring — the risk of hitting a female with kits.
- Do not try to pull an animal out of a trap without covering it with a blanket or burlap bag. A scared marten will go through any gap that appears while handling the cage — and it will bite on the way.
- Do not approach an animal that looks sick or injured. On the contrary — move away and call the nearest wild animal rehabilitation center. Rabies and other diseases change a marten's behavior in deceptive ways: it may seem tame, gentle, or trusting. It's a trap.
- Do not separate fighting animals with your hands. A garden hose with a strong stream of water, noise (clapping, whistling), a broom held by the long end — all are more effective and safer than a forearm between a dog and a marten.
- Focus on prevention instead of catching — secure the attic with 2 cm mesh, the chicken coop with 6 mm, and use a closed composter. A full overview of solutions is in the marten and weasel deterrence guide and in the text what traps to use for weasels and martens (if you must catch — do it safely and legally).
One must also keep proportions in mind. A marten is not an aggressor hunting humans — it is an opportunistic predator with a flight distance of several meters. In normal conditions, it simply avoids you. Its role in the local ecosystem is actually important, as we write in the text about the role of martens and weasels in the ecosystem. A bite happens when a human violates this distance rule — in panic, out of curiosity, or with good rescue intentions. Each of these situations is avoidable.
Bitten by a marten? Stay calm. Wash with soap and water for 15 minutes, apply antiseptic (octenidine or povidone-iodine), use a loose dressing, and take photos of the wound. Tetanus — booster if 5+ years have passed. Rabies — a doctor assesses this; if the animal escaped or looked sick, go to the ER. Face, hand, child, or animal bitten by a marten — see a specialist on the same day without discussion. Most incidents end after 7–10 days with an invisible mark; the key is the first 15 minutes and one decision: don't wait.
★Frequently asked questions
Is a marten bite dangerous?
Yes, every bite from a wild mammal is potentially dangerous, although the marten is not a particularly lethal species. The three main risks are: bacterial infection (most commonly Pasteurella multocida, phlegmon, and in extreme cases sepsis), tetanus (if vaccination is not up to date), and rabies (rare in Poland but real — especially in eastern provinces; once symptoms appear, the disease is 100% fatal). First aid (15 minutes of washing with soap and water, antiseptic) and medical consultation reduce the risk of serious complications to a minimum.
Do I have to go to the ER after a marten bite?
Absolutely yes, if: the wound is on the face, hand, or joint; the victim is a child, pregnant woman, or immunocompromised; bleeding is difficult to stop; the animal escaped or looked sick (rabies PEP risk); symptoms of infection appear (fever, increasing swelling, pus, red streaks). For a small superficial bite on a healthy adult with an up-to-date tetanus vaccination, a visit to a GP within 24 hours is sufficient, but medical consultation is standard, not over-caution.
How to disinfect a wound after a marten bite?
First, 15 minutes of washing with soap and water under running water — this is the most important part of the entire procedure and nothing replaces it. Then use an antiseptic: octenidine with phenoxyethanol (Octenisept, Octenilin) or povidone-iodine (Betadine) — both available over the counter. Alcohol and hydrogen peroxide are less recommended as they irritate tissues and slow healing. Finally, apply a loose, non-occlusive dressing of sterile gauze. Do not seal the wound tightly and do not use hydrocolloid plasters — anaerobes (including tetanus) multiply without access to air.
Can a marten have rabies?
Yes, although it's rare. Mustelids (stone marten, pine marten, weasel, polecat) are sometimes described as carriers of the rabies virus, usually secondarily after foxes. Poland is not officially a rabies-free country for wild animals; cases are recorded every few years in some provinces (mainly eastern). Every bite by a wild animal is treated by default as a potential exposure until a doctor decides otherwise. Post-exposure prophylaxis (PEP) — a 5-dose schedule (days 0, 3, 7, 14, 28), possibly with immunoglobulin — implemented within 24–48 hours protects 100%.
What to do when a marten has bitten a dog or cat?
See a veterinarian on the same day, regardless of how the wound looks. Before transport: safely separate the animals, assess the general condition (breathing, gait, bleeding), rinse the wound with saline or boiled water (not human antiseptics — some irritate animal mucous membranes), apply a light protective dressing, and transport in a carrier. At the clinic: surgical debridement, antibiotic therapy, and vaccine assessment. If the dog/cat does not have an up-to-date rabies vaccination, the regional veterinarian will impose mandatory observation for up to 6 months.
After how many years should a tetanus booster be given?
In adults, a booster dose every 10 years (Td or Tdap preparation) is recommended. After a bite, a shortened scheme applies: vaccination less than 5 years ago — usually no additional dose for a clean wound; vaccination 5–10 years ago — booster dose; vaccination more than 10 years ago or not remembered — booster dose, and for deep bite wounds, additional tetanus immunoglobulin. If there is no documented vaccination at all — a full primary vaccination schedule plus immunoglobulin. The decision is made by a doctor; it is worth bringing your vaccination card or records from previous visits.


